English
English
9:30 a.m.
Patient Arrives to ED
A 63-year-old male with a history of coronary artery disease, diabetes and lung cancer presents to the ED complaining of generalized body aches and weakness, which had started about one week prior.
Patient denies localized weakness or numbness, chest pain, shortness of breath, abdominal pain, headache, or urinary symptoms. his last chemotherapy was the month prior.
Patient is thrombocytopenic
Chief Complaint:
Fatigue, intermittent nausea, worsening chills mostly at night times
9:35 a.m.
Vital Signs are Assessed
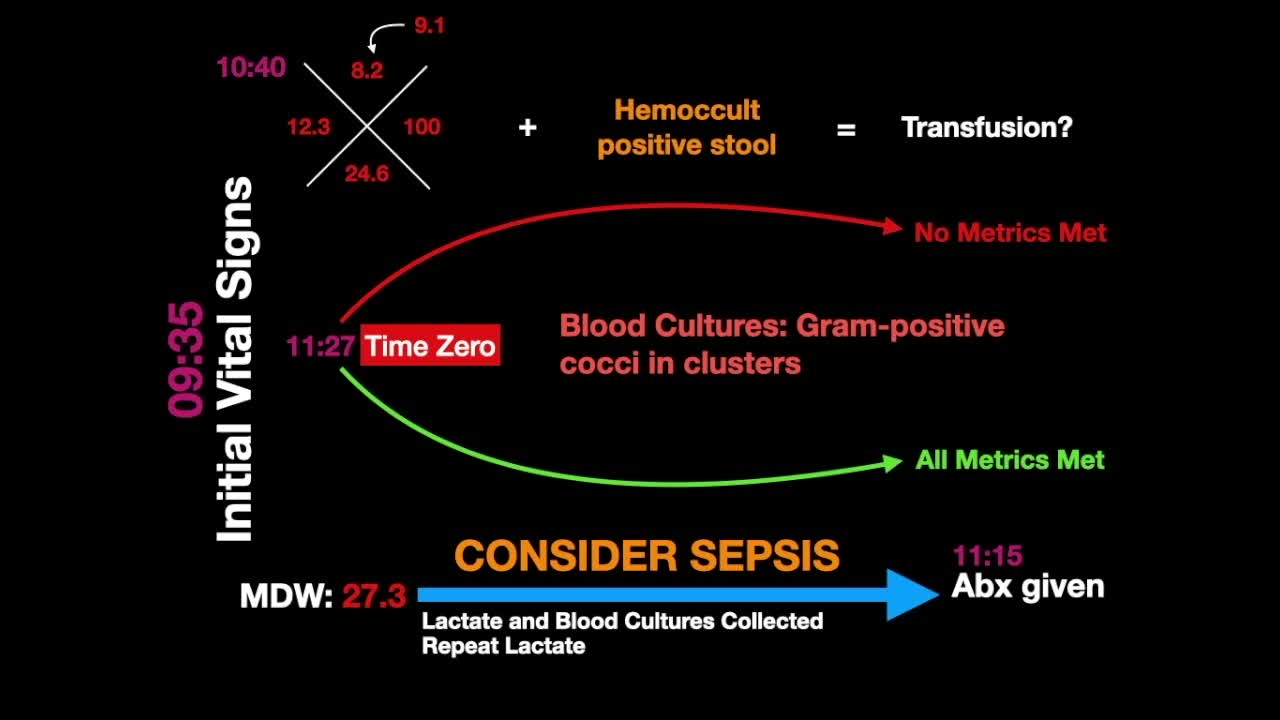
The initial vital signs are assessed:
- Temperature: 37.1°C (98.8°F)
- Blood pressure: 122/73
- Pulse: 88
- Respiratory rate: 21
- SpO2: 97% (RA)
Mildly dry mucous membranes and hemoccult-positive stool.
10:40 a.m.
CBC with differential and MDW results
Slightly elevated WBC at 12.3
Anemia with hemoglobin of 8.2, decrease from a previous measurement of 9.1 taken approximately two months prior.
MDW results of 27.3 come in.
10:45 a.m.
Severe infection and sepsis added to differential diagnosis and additional tests ordered
Based on the elevation of WBC and MDW levels, the physician adds severe infection and risk of sepsis to differential diagnosis. Ordered head to toe exam and sepsis panel: lactate, blood cultures and antibiotics.
What are we missing?
A head-to-toe exam reveals mild erythema and induration around the Portacath, suggesting a port site infection.
11:15 antibiotics are given
11:27 a.m.
Sepsis Time Zero - SEP-1 Metrics Met
Lactate 3.2
- Note: Days later, blood cultures grew gram-positive cocci in clusters, suggestive of staph from an infected port site